Dermatomyositis (DM) is an autoimmune disease characterized primarily by proximal muscle weakness and skin changes (such as Gottron papules and heliotrope rash). Other associated diseases include interstitial lung disease and arthritis. DM may also represent a paraneoplastic phenomenon in a subset of cases. A variety of autoantibodies are associated with DM such as Anti-Mi2, Anti-Jo 1, and Anti-P155/ P140. Muscle injury occurs due to immunologic damage to small blood vessels with deposition of complement membrane attack complex (C5b-9). Corticosteroids are the first-line therapy for DM.
The characteristic features of DM are seen in this case. Routine H&E sections show myocyte perifascicular atrophy as well as scattered regenerating fibres and necrotic fibres. The proportion of myocytes having internalized nuclei is increased (greater than 5%). There is also moderate, patchy fibrosis and edema of the interstitium with multiple foci of significant mononuclear endomysial inflammation. The vasculature shows a spectrum of changes from endomysial capillary loss to perivascular inflammatory foci.
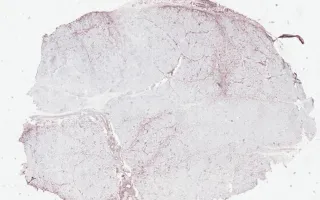
Immunohistochemistry for MHC show upregulation at the edge of the fascicles. C5b-9 staining is positive in many endomysial capillaries and myocytes, especially in perifascicular distribution.
This slide shows MHC stain. See related content for H&E and C5b-9 stains.
Yang, H., Keith, J. Muscle, Dermatomyositis, MHC stain. Digital Laboratory Medicine Library, Dept of Laboratory Medicine & Pathobiology, University of Toronto. Published
. Accessed December 17, 2025. https://dev.dlml.cflabs.ca/image/muscle-dermatomyositis-mhc-stain-lmp11398