Details
Lymph node excision – requesting lymphoma protocol.
Follicular hyperplasia is a reactive pattern reflecting a stimulation of the B-cell compartment within a lymph node.
This is a relatively enlarged lymph node, although larger lymph nodes are often seen, depending on the anatomical region (e.g. inguinal, thoracic). Identification of the specimen as a lymph node is sometimes not straight forward, and "lymphoid tissue" may be more accurate in some cases. In this specimen, the identification of the capsule and sinusoids is helpful. The medulla cannot be clearly identified, possibly related to the orientation of the cut.
The sections show increased number of secondary follicles, but with preserved architecture. Closer look at the germinal centres show the presence of centrocytes, centroblasts and tingible body macrophages; this makeup drastically differs from that of a proliferation centre seen in B-cell lymphomas.
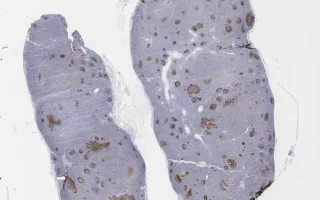
The follicles also show polarity—a feature absent in malignant processes. This is often highlighted when examining the MIB1 stain.
BCL-2 interpretation can be challenging at times; it is prudent to remember that T-cells express BCL-2. It is important to interpret these cases in the context of T-cell markers (CD3, CD5).
CD21 and CD23 are used to examine the follicular dendritic network. While some follicles do appear abnormally expanded, examining the follicular network helps to guide the diagnosis.
Follicular hyperplasia may be caused by bacteria, rheumatoid arthritis, virus (HIV) or associated with Castleman's disease.
This slide shows MIB1 stain. See related content for H&E, CD3, BCL-2, CD20, and CD21 stains.