History of multiple previous uterine dilatation and curettages.
Case Discussion
The pathological basis of abnormal placental attachment stems from a partial or complete loss of maternal decidua such that chorionic villi are adjacent to or actually extending into uterine myometrium.
Three gradations of this entity are recognized:
a. Placenta accreta vera – when villi are attached to but do invade underlying myometrium
b. Placenta increta – when villi show infiltration within but not through the myometrium
c. Placenta percreta – when the entire myometrium and possibly the uterine serosa is penetrated by chorionic villi, with possible extension into neighboring organs (ex. bladder, bowel).
Risk factors for all forms of abnormal placental attachment include history of uterine trauma (cesarean section, dilatation and curettage, manual placental extraction, myomectomy), abnormal placenta location (previa, cornual implantation), abnormal uterine anatomy (malformations, tumours), advanced maternal age, and multiparity. In general, the occurrence of this entity is rare in an unscarred uterus.
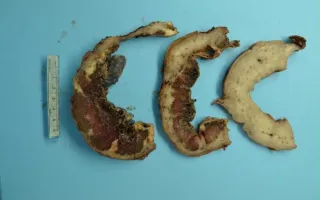
This patient had a history of multiple dilatation and curettages. The placenta was also located such that it partially covered the cervical os (partial previa). Radiologically, placenta percreta was suspected with potential involvement of the urinary bladder. Hysterectomy was performed following cesarean section. On gross sections through the uterus and placenta, brown placental parenchyma is seen extending through the entirety of the tan myometrium to the serosal surface of the uterus. The fetal surface can be identified by its grey-purple colour and vessels.
Hodgson, A., Keating, S. Placenta, Abnormal placental attachment. Digital Laboratory Medicine Library, Dept of Laboratory Medicine & Pathobiology, University of Toronto. Published
. Accessed December 17, 2025. https://dev.dlml.cflabs.ca/image/placenta-abnormal-placental-attachment-lmp22594