Acute neurological deterioration with absent motor and sensory responses in the face, arms, and legs on nerve conduction studies and electromyogram. Suspicion of Guillain-Barré syndrome/acute motor and sensory axonal neuropathy. Left lower leg muscle biopsy.
Case Discussion
Inflammatory polyneuropathies such as Guillain-Barré syndrome can lead to loss of innervation and muscle injury.
Muscle injury can be broadly classified based on two mechanisms: 1) myopathic injury (direct damage to myofibers), and 2) neurogenic injury (from disruption of muscle innervation). Neurogenic injury is characterized by increased variability in the size and shape of myocytes - with atrophy occurring in clusters (grouped atrophy) - and myofibers which take on an angulated shape.
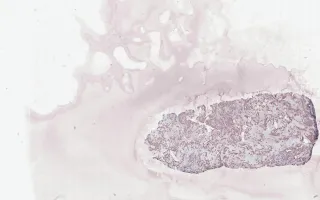
Grouping of fiber types with loss of the normal checkerboard distribution on immunohistochemistry for myosin S and myosin F is a diagnostic feature of neurogenic injury. This case also shows a predominance of type I fibers and selective atrophy of type II fibers which can be seen in prolonged corticosteroid use, muscle disuse, and denervation.
This slide shows myosin F stain. See Related Content for H&E and myosin S stains.
Yang, H., Keith, J. Muscle, Denervation atrophy secondary to polyneuropathy, myosin F stain. Digital Laboratory Medicine Library, Dept of Laboratory Medicine & Pathobiology, University of Toronto. Published
. Accessed December 17, 2025. https://dev.dlml.cflabs.ca/image/muscle-denervation-atrophy-secondary-polyneuropathy-myosin-f-stain-lmp39850